Learn more about the Respiratory System
In this module, you will learn more about
- Respiratory system function
- Structure of the respiratory system
- The mechanics of pulmonary ventilation
- Lung tissue compliance
- Control of normal pulmonary ventilation is driven by carbon dioxide
- Partial pressure and gas exchange
- External and internal respiration
Learn even more: See Chemistry, Tissues and Cardiovascular modules
1 Respiratory system function
Most of our metabolic needs require adenosine triphosphate (ATP). ATP synthesis requires oxygen and generates carbon dioxide. Our cells therefore require oxygen to carry-out vital functions. The primary function of the respiratory system is to supply the body with oxygen and to excrete carbon dioxide. It also has several other functions:
The purpose of this module is to focus on gas exchange (oxygen and carbon dioxide), which involves;
- Communication (speech)
- Olfaction (the sense of smell)
- Acid-base balance (short-term control by eliminating carbon dioxide).
- Blood pressure (BP) maintenance through the synthesis of angiotensin II
- Blood and lymph flow; breathing creates a pressure gradient that promotes this flow
- Blood filtration by filtering small clots from the vascular system
- Expulsion of abdominal contents; holding one’s breath helps eliminate urine, faeces and the foetus during childbirth.
The purpose of this module is to focus on gas exchange (oxygen and carbon dioxide), which involves;
- Pulmonary ventilation
- External respiration
- Transport of respiratory gases
- Internal respiration
2 Structure of the respiratory system
|
|
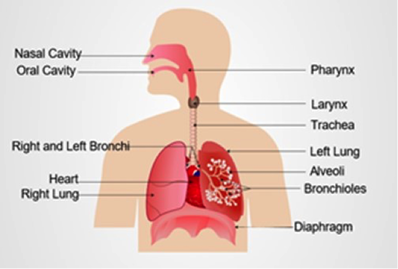
Structure of the respiratory system (depositphotos.com)
|
The right lung contains three lobes and the left lung contains only two in order to accommodate the heart in the thoracic cavity.
The respiratory system starts at the nostrils, where air enters the nose during inspiration, travels via the pharynx, the larynx, and the trachea. The trachea divides into the right and left bronchi (singular - bronchus) which enter the lungs. Air then moves through smaller and smaller passageways known as bronchioles, until it enters tiny air sacs known as alveoli (singular - alveolar), which are the main structural feature of the lungs, and the major site for gas exchange.
As inhaled air (inspiration), moves along the respiratory tract it is moistened and warmed, and small particles are trapped so as not to enter the lungs. Once gas exchange has occurred the air moves back through the tract and is expelled (expiration).
Functionally, the respiratory system is divided into two parts: the conducting zone and the respiratory zone. The conducting zone consists of all passageways through which air moves without gas exchange taking place, that is from the nostrils through to the smallest terminal bronchioles. The respiratory zone is the site of gas exchange and consists of the respiratory bronchioles and the alveoli.
The respiratory system starts at the nostrils, where air enters the nose during inspiration, travels via the pharynx, the larynx, and the trachea. The trachea divides into the right and left bronchi (singular - bronchus) which enter the lungs. Air then moves through smaller and smaller passageways known as bronchioles, until it enters tiny air sacs known as alveoli (singular - alveolar), which are the main structural feature of the lungs, and the major site for gas exchange.
As inhaled air (inspiration), moves along the respiratory tract it is moistened and warmed, and small particles are trapped so as not to enter the lungs. Once gas exchange has occurred the air moves back through the tract and is expelled (expiration).
Functionally, the respiratory system is divided into two parts: the conducting zone and the respiratory zone. The conducting zone consists of all passageways through which air moves without gas exchange taking place, that is from the nostrils through to the smallest terminal bronchioles. The respiratory zone is the site of gas exchange and consists of the respiratory bronchioles and the alveoli.
The Conducting Zone
The conducting zone includes:
Further subdivisions result in the formation of bronchioles (1mm diameter) and then terminal bronchioles (0.5mm diameter).
As the conducting tubes become smaller and smaller less and less cartilage is apparent and the walls of the bronchioles contain elastic cartilage. Mucosal epithelium and cilia become sparse and the amount of smooth muscle increases. Alveolar macrophages take over the role of foreign particle removal.
This division of the air passageways occurs up to 23 times and it is known as the bronchiole tree. The final subdivision results in the formation of the respiratory bronchioles that are the beginning of the respiratory zone.
- The nose - air is warmed, moistened, and due to air turbulence air makes contact with mucosal surfaces where particulate matter becomes trapped
- The pharynx - connects the nasal cavity and the mouth superiorly to the larynx.
- The larynx - a cartilaginous structure about 5 cm long, and functions to provide an open airway, while keeping food and drink out of the airway. The larynx is continuous with the trachea.
- The trachea - approximately 12 cm long lying anteriorly to the oesophagus. Structurally the trachea consists of C-shaped rings of hyaline cartilage which stops it from collapsing during inhalation. Mucous secreting goblet cells trap inhaled particles while cilia drives mucous up (acts as a respiratory escalator) towards the pharynx, where it can be swallowed.
- The carina – where the trachea divides into the right and left bronchi. The carina is highly sensitive and promotes coughing when foreign particles make contact with it.
- Secondary bronchi - once inside the lungs the bronchi subdivide into secondary bronchi, one to each lung lobe.
Further subdivisions result in the formation of bronchioles (1mm diameter) and then terminal bronchioles (0.5mm diameter).
As the conducting tubes become smaller and smaller less and less cartilage is apparent and the walls of the bronchioles contain elastic cartilage. Mucosal epithelium and cilia become sparse and the amount of smooth muscle increases. Alveolar macrophages take over the role of foreign particle removal.
This division of the air passageways occurs up to 23 times and it is known as the bronchiole tree. The final subdivision results in the formation of the respiratory bronchioles that are the beginning of the respiratory zone.
The respiratory zone
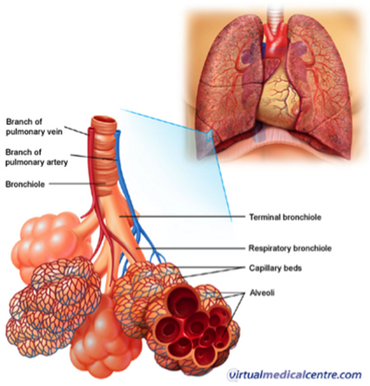
The respiratory zone, showing the respiratory bronchioles and alveoli. http://www.virtualcancercentre.com/uploads/VMC/DiseaseImages/2293_alveoli_450.jpg
The respiratory zone consists of the respiratory bronchiole, the alveolar ducts and the alveoli.
95 % of the alveolar surface is composed of a single layer of squamous epithelium (Type I cells). These cells are numerous and provide a huge surface area for gas exchange. The other 5 % of the alveolar surface is composed of Type II cells, which secrete pulmonary surfactant and prevent the alveoli from collapsing on exhalation. A thin film of moisture covers the alveolar wall, and fine elastic fibres and blood capillaries surround the outer surface of each alveolar sac. There are some 300 million alveoli in a set of mature lungs creating an enormous surface area for gas exchange.
Maturation of the alveoli begins in utero around 8 months gestation and continues into childhood. A full complement of alveoli are not present until around 8 years of age.
The respiratory gas exchange membrane is made up of 4 layers of cells. On the inside of the alveoli is the squamous cell layer supported by its tissue basement membrane. Next to this, is the capillary basement membrane and the internal (endothelial) cell layer of the capillary. This thin set of layers creates the distance through which gas exchange must occur and so is referred to as the diffusion distance.
95 % of the alveolar surface is composed of a single layer of squamous epithelium (Type I cells). These cells are numerous and provide a huge surface area for gas exchange. The other 5 % of the alveolar surface is composed of Type II cells, which secrete pulmonary surfactant and prevent the alveoli from collapsing on exhalation. A thin film of moisture covers the alveolar wall, and fine elastic fibres and blood capillaries surround the outer surface of each alveolar sac. There are some 300 million alveoli in a set of mature lungs creating an enormous surface area for gas exchange.
Maturation of the alveoli begins in utero around 8 months gestation and continues into childhood. A full complement of alveoli are not present until around 8 years of age.
The respiratory gas exchange membrane is made up of 4 layers of cells. On the inside of the alveoli is the squamous cell layer supported by its tissue basement membrane. Next to this, is the capillary basement membrane and the internal (endothelial) cell layer of the capillary. This thin set of layers creates the distance through which gas exchange must occur and so is referred to as the diffusion distance.
The lungs
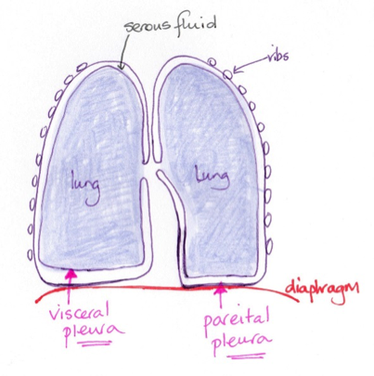
© Dr Patricia Logan 2017: The lungs
The surface of the lungs is covered with serous membrane, the visceral pleura.
This visceral pleura turns back on itself and forms the parietal pleura, which is attached to the mediastinum and the superior surface of the diaphragm.
Between the two pleural layers is a space, the pleural cavity, containing slippery pleural fluid.
The pleura and pleural fluid serve to reduce friction during breathing and compartmentalise the lungs within the thoracic cavity. The fluid keeps the two layers in contact with each other to create a pressure gradient for airflow. As the ribs and diaphragm are moved, the layers of pleura move with them expanding the lung tissue and consequently decreasing the pressure of air within the alveoli.
Excess fluid between the pleural layers due to inflammation or scarring of the pleura can inhibit the capacity of the lungs to expand.
This visceral pleura turns back on itself and forms the parietal pleura, which is attached to the mediastinum and the superior surface of the diaphragm.
Between the two pleural layers is a space, the pleural cavity, containing slippery pleural fluid.
The pleura and pleural fluid serve to reduce friction during breathing and compartmentalise the lungs within the thoracic cavity. The fluid keeps the two layers in contact with each other to create a pressure gradient for airflow. As the ribs and diaphragm are moved, the layers of pleura move with them expanding the lung tissue and consequently decreasing the pressure of air within the alveoli.
Excess fluid between the pleural layers due to inflammation or scarring of the pleura can inhibit the capacity of the lungs to expand.
3 The mechanics of pulmonary ventilation
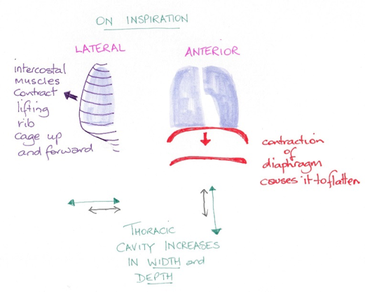
© Dr Patricia Logan 2017: Pulmonary ventilation
Pulmonary ventilation (breathing), consists of a continuous cycle of inspiration and expiration.
One inspiration and one expiration is known as the respiratory cycle. Respiration can be either quiet, as when one is at rest, or forced, for example during exercise.
In order to breathe, muscles, in particular the intercostal muscles and the diaphragm, expand and contract the thoracic cavity.
During inspiration, the diaphragm contracts downwards and the external intercostal muscles cause the rib cage to rise thus expanding the lungs. Due to an increase in the volume of the lungs the air pressure falls below that of atmospheric pressure, reducing the air pressure inside the lungs. Air moves down its concentration gradient and into the lungs. Inspiration is an active process.
During the passive process of expiration, dependent on the elastic recoil of the lungs, the diaphragm relaxes and rises, the rib cage descends and the volume inside the lungs decreases. The air pressure inside the lungs increases above atmospheric pressure and air moves down its concentration gradient and out of the lungs.
One inspiration and one expiration is known as the respiratory cycle. Respiration can be either quiet, as when one is at rest, or forced, for example during exercise.
In order to breathe, muscles, in particular the intercostal muscles and the diaphragm, expand and contract the thoracic cavity.
During inspiration, the diaphragm contracts downwards and the external intercostal muscles cause the rib cage to rise thus expanding the lungs. Due to an increase in the volume of the lungs the air pressure falls below that of atmospheric pressure, reducing the air pressure inside the lungs. Air moves down its concentration gradient and into the lungs. Inspiration is an active process.
During the passive process of expiration, dependent on the elastic recoil of the lungs, the diaphragm relaxes and rises, the rib cage descends and the volume inside the lungs decreases. The air pressure inside the lungs increases above atmospheric pressure and air moves down its concentration gradient and out of the lungs.
4 Lung tissue compliance
The ability of the lungs to expand is known as lung compliance.
The higher the compliance, the easier it is to expand the lungs.
Compliance is determined by the distensibility of lung tissue and the alveolar surface tension.
Healthy lungs generally have high compliance, they distend easily and the alveolar surface tension is low. Loss of elasticity of the lungs, due to inflammation or infection, development of scar tissue or decreased production of surfactant, decreases lung compliance making it more difficult to breathe. Furthermore, if thoracic cavity compliance is low, for example, due to damage to the intercostal muscles making it difficult to move the rib cage, lung compliance will be impeded.
So, compliance of the respiratory system is comprised of lung tissue compliance and thoracic cavity compliance. Damage to either will affect the ability to breathe.
The higher the compliance, the easier it is to expand the lungs.
Compliance is determined by the distensibility of lung tissue and the alveolar surface tension.
Healthy lungs generally have high compliance, they distend easily and the alveolar surface tension is low. Loss of elasticity of the lungs, due to inflammation or infection, development of scar tissue or decreased production of surfactant, decreases lung compliance making it more difficult to breathe. Furthermore, if thoracic cavity compliance is low, for example, due to damage to the intercostal muscles making it difficult to move the rib cage, lung compliance will be impeded.
So, compliance of the respiratory system is comprised of lung tissue compliance and thoracic cavity compliance. Damage to either will affect the ability to breathe.
5 Control of Normal Pulmonary Ventilation is Driven by Carbon Dioxide
|
|
|
Within two areas of the medulla oblongata, in the brainstem, are neurons that are important for respiration; the ventral respiratory groups (VRG) and the dorsal respiratory group (DRG). These neurons control respiratory rhythm.
The DRG monitors and integrates information from peripheral stretch receptors and chemoreceptors, and relays this information to the VRG.
The pontine respiratory centre, located in the pons, transmits impulses to the VRG and modifies the actions of the medullary neurons during times of speech, sleep, and exercise.
The rate and depth of breathing is controlled by several factors which either stimulate or inhibit the respiratory centres in the medulla oblongata and the pons.
Chemical factors that affect breathing rate include the levels of carbon dioxide, oxygen and hydrogen in arterial blood. Levels of carbon dioxide are the most significant factor controlling the rate and depth of breathing. The partial pressure (PP) of carbon dioxide in arterial blood is approximately 40 mmHg. Homeostasis is maintained by the chemoreceptors that sense carbon dioxide levels.
When carbon dioxide levels rise in the blood (hypercapnia), the gas accumulates in the brain. The carbon dioxide becomes hydrated forming carbonic acid and hydrogen ions. This release of hydrogen ions causes a drop in pH (increase in acidity), which leads to an increase in alveolar ventilation. The rate and depth of breathing increases, more carbon dioxide is exhaled and the pH rises.
If the rate and depth of breathing increases in the absence of high carbon dioxide levels (as in panic attacks), carbon dioxide levels fall (hypocapnia), and the pH rises (more alkaline). This results in constriction of cerebral blood vessels and poor perfusion of the brain. If carbon dioxide becomes abnormally low then respiration may be inhibited and can lead to the cessation of breathing (apnea).
Other factors that affect the rate and depth of breathing are arterial blood oxygen levels, and arterial pH. Oxygen levels only have a small effect on pulmonary ventilation. Oxygen levels must drop significantly before this gas becomes a stimulus for ventilation.
- The VRG – fires on inspiration.
- The DRG – fires on expiration.
The DRG monitors and integrates information from peripheral stretch receptors and chemoreceptors, and relays this information to the VRG.
The pontine respiratory centre, located in the pons, transmits impulses to the VRG and modifies the actions of the medullary neurons during times of speech, sleep, and exercise.
The rate and depth of breathing is controlled by several factors which either stimulate or inhibit the respiratory centres in the medulla oblongata and the pons.
Chemical factors that affect breathing rate include the levels of carbon dioxide, oxygen and hydrogen in arterial blood. Levels of carbon dioxide are the most significant factor controlling the rate and depth of breathing. The partial pressure (PP) of carbon dioxide in arterial blood is approximately 40 mmHg. Homeostasis is maintained by the chemoreceptors that sense carbon dioxide levels.
When carbon dioxide levels rise in the blood (hypercapnia), the gas accumulates in the brain. The carbon dioxide becomes hydrated forming carbonic acid and hydrogen ions. This release of hydrogen ions causes a drop in pH (increase in acidity), which leads to an increase in alveolar ventilation. The rate and depth of breathing increases, more carbon dioxide is exhaled and the pH rises.
If the rate and depth of breathing increases in the absence of high carbon dioxide levels (as in panic attacks), carbon dioxide levels fall (hypocapnia), and the pH rises (more alkaline). This results in constriction of cerebral blood vessels and poor perfusion of the brain. If carbon dioxide becomes abnormally low then respiration may be inhibited and can lead to the cessation of breathing (apnea).
Other factors that affect the rate and depth of breathing are arterial blood oxygen levels, and arterial pH. Oxygen levels only have a small effect on pulmonary ventilation. Oxygen levels must drop significantly before this gas becomes a stimulus for ventilation.
6 Partial pressure and gas exchange
In order to understand gas exchange between the alveoli and the blood, and the blood and tissues one needs to understand partial pressure (PP), of gases.
Air is composed of approximately 78.6 % nitrogen, 20.9 % oxygen, 0.04 % carbon dioxide, several other gases in miniscule amounts, and water vapour.
The contribution of all these gases make up total atmospheric pressure of 760 mmHg at sea level.
Each gas contributes to atmospheric pressure such that in the case of oxygen then 20.9 % of the atmospheric pressure is oxygen. This contribution of oxygen to atmospheric pressure is known as the partial pressure.
20.9/100 x 760mmHg = 158.84 mmHg ... so the PP of oxygen is therefore 159 mmHg.
Likewise, carbon dioxide contributes 0.04 % to atmospheric pressure.
0.04/100 x 760mmHg = 0.3mmHg ... so the PP of carbon dioxide in the atmosphere is 0.3 mmHg
For further information on PP, investigate Dalton’s Law.
The composition of air inhaled changes in the alveoli due to humidification, mixing with residual air from the previous respiratory cycle, and alveolar gas exchange; oxygen moves into the blood and carbon dioxide moves from the blood into the alveoli. As a consequence, the PP of the gases change in the alveoli, this is important for the movement of respiratory gases into and out of the blood.
The respective PP in inspired air:
The PP in alveolar air:
Note that in the alveoli the PP of oxygen is about 65 % of its partial pressure in the atmosphere, and the partial pressure of carbon dioxide has increased about 130 times.
Air is composed of approximately 78.6 % nitrogen, 20.9 % oxygen, 0.04 % carbon dioxide, several other gases in miniscule amounts, and water vapour.
The contribution of all these gases make up total atmospheric pressure of 760 mmHg at sea level.
Each gas contributes to atmospheric pressure such that in the case of oxygen then 20.9 % of the atmospheric pressure is oxygen. This contribution of oxygen to atmospheric pressure is known as the partial pressure.
20.9/100 x 760mmHg = 158.84 mmHg ... so the PP of oxygen is therefore 159 mmHg.
Likewise, carbon dioxide contributes 0.04 % to atmospheric pressure.
0.04/100 x 760mmHg = 0.3mmHg ... so the PP of carbon dioxide in the atmosphere is 0.3 mmHg
For further information on PP, investigate Dalton’s Law.
The composition of air inhaled changes in the alveoli due to humidification, mixing with residual air from the previous respiratory cycle, and alveolar gas exchange; oxygen moves into the blood and carbon dioxide moves from the blood into the alveoli. As a consequence, the PP of the gases change in the alveoli, this is important for the movement of respiratory gases into and out of the blood.
The respective PP in inspired air:
- Oxygen 159 mmHg
- Carbon dioxide 0.3 mmHg
The PP in alveolar air:
- Oxygen 104 mmHg
- Carbon dioxide 40 mmHg
Note that in the alveoli the PP of oxygen is about 65 % of its partial pressure in the atmosphere, and the partial pressure of carbon dioxide has increased about 130 times.
7 External and internal respiration
External respiration
The alveoli epithelium is covered in a thin layer of water through which oxygen diffuses, cross the respiratory membrane and enter the blood. Carbon dioxide moves in the opposite direction, across the same surfaces, to enter the alveoli. This is alveolar gas exchange or external respiration. Both oxygen and carbon dioxide move down their partial pressure gradients, that is from areas of higher partial pressure to areas of lower partial pressure.
The PP of oxygen is 104 mmHg in the alveoli and 40 mmHg in the blood returning to the lungs. Oxygen therefore moves from the alveoli into the blood. For carbon dioxide, the PP in the alveoli is 40 mmHg and in the blood, returning to the lungs, 45 mmHg. Carbon dioxide therefore moves from the blood into the alveoli.
Other factors that affect the movement of these two gases across the respiratory membrane include;
The PP of oxygen is 104 mmHg in the alveoli and 40 mmHg in the blood returning to the lungs. Oxygen therefore moves from the alveoli into the blood. For carbon dioxide, the PP in the alveoli is 40 mmHg and in the blood, returning to the lungs, 45 mmHg. Carbon dioxide therefore moves from the blood into the alveoli.
Other factors that affect the movement of these two gases across the respiratory membrane include;
- The solubility of the gases. Carbon dioxide is about 20 times more soluble than oxygen (carbon dioxide diffuses through water more easily), which means that while oxygen has a greater pressure gradient, equal amounts of each gas are exchanged.
- Thickness of the respiratory membrane
- Surface area of the lungs.
Ventilation-perfusion coupling
In the lungs blood flow to the alveoli is matched to areas of maximal ventilation.
Vasoconstriction will occur in areas where ventilation is poor, re-routing blood to areas with better ventilation and hence higher oxygen partial pressure. The higher oxygen level will cause vasodilation of the capillary bed in this region of the lung promoting blood uptake of oxygen and removal of carbon dioxide.
These changes also stimulate bronchoconstriction or dilation, thus adjusting ventilation, and airflow to better blood perfused areas of the lungs.
NOTE: This is the opposite of what happens for oxygen delivery at the tissue–capillary interface
Vasoconstriction will occur in areas where ventilation is poor, re-routing blood to areas with better ventilation and hence higher oxygen partial pressure. The higher oxygen level will cause vasodilation of the capillary bed in this region of the lung promoting blood uptake of oxygen and removal of carbon dioxide.
These changes also stimulate bronchoconstriction or dilation, thus adjusting ventilation, and airflow to better blood perfused areas of the lungs.
NOTE: This is the opposite of what happens for oxygen delivery at the tissue–capillary interface
Transport of respiratory gases
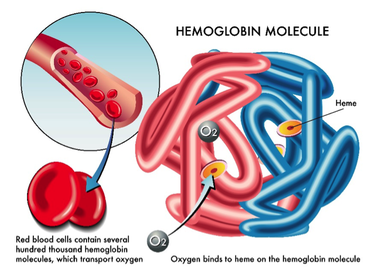
Structure of a haemoglobin molecule (depositphotos.com)
The loading and unloading of oxygen and carbon dioxide respectively, involves erythrocytes (red blood cells, RBCs) and the blood, which transports oxygen to the tissues and returns carbon dioxide to the lungs to be excreted.
Oxygen transport (approximately):
Haemoglobin consists of four protein chains (two alpha and 2 beta chains), each containing a haem group that contains an iron atom at its centre. Each iron atom can bind one oxygen molecule, so each haemoglobin can carry up to 4 oxygen molecules. One RBC can carry one billion moledules of oxygen on about 280 million haemoglobin molecules. When no oxygen is bound, it is known as deoxyhaemoglobin. If four oxygen molecules are bound to one haemoglobin molecule it is considered saturated and no more oxygen can bind.
Carbon dioxide transport (approximately):
Note: the smaller the amount of oxygen being carried by a haemoglobin molecule the more carbon dioxide it can carry and vice versa. This is known as the Haldane Effect and assists in transport of carbon dioxide from the tissues back to the lungs.
Oxygen transport (approximately):
- 98.5% bound to haemoglobin (oxyhaemoglobin) within RBCs
- 1.5% dissolved in plasma
Haemoglobin consists of four protein chains (two alpha and 2 beta chains), each containing a haem group that contains an iron atom at its centre. Each iron atom can bind one oxygen molecule, so each haemoglobin can carry up to 4 oxygen molecules. One RBC can carry one billion moledules of oxygen on about 280 million haemoglobin molecules. When no oxygen is bound, it is known as deoxyhaemoglobin. If four oxygen molecules are bound to one haemoglobin molecule it is considered saturated and no more oxygen can bind.
Carbon dioxide transport (approximately):
- 70 % carbon dioxide is transported as bicarbonate ion dissolved in RBC cytoplasm or plasma
- 23% is bound to globin protein chains of haemoglobin
- 7 % is dissolved in the blood
Note: the smaller the amount of oxygen being carried by a haemoglobin molecule the more carbon dioxide it can carry and vice versa. This is known as the Haldane Effect and assists in transport of carbon dioxide from the tissues back to the lungs.
Internal respiration
Internal respiration takes place at the capillary-tissue interface where carbon dioxide moves out of the tissues and into the blood, to be returned to the lungs, and oxygen moves out of the blood and into the tissues. Both gases move down their pressure gradients just as they did during external respiration, but in the opposite direction.
PP in oxygenated blood:
PP in the tissues and deoxygenated blood:
PP in oxygenated blood:
- Oxygen 100 mmHg
- Carbon dioxide 40 mmHg
PP in the tissues and deoxygenated blood:
- Oxygen < 40 mmHg
- Carbon dioxide 45 mmHg
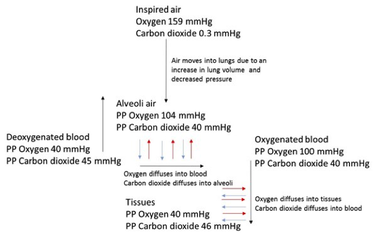
© Judith Salvage-Jones 2017: A summary of internal and external respiration
Respiratory gases are thus exchanged at the alveoli-blood interface and at the capillary-tissue interface by simple diffusion, each gas moving down its concentration gradient, in opposing directions.

